Catamaran Prior Prescription (Rx) Authorization Form

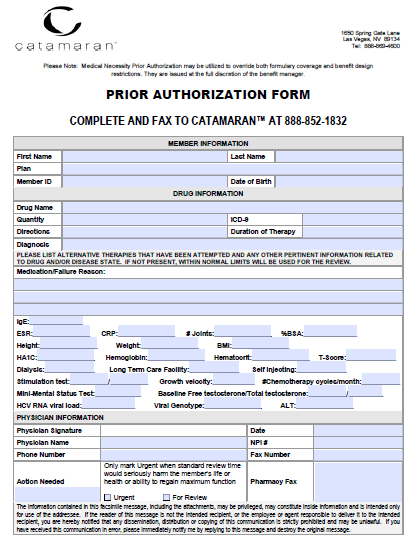
The Catamaran Prior Prescription Authorization Form allows beneficiaries of Catamaran health insurance to receive coverage for a prescription drug which is not on the formulary or not customarily prescribed as the primary treatment option. The prescriber should be the healthcare professional managing the patient’s symptoms and condition, and the form should be completed by this individual with a full justification for the request including all treatments attempted prior to completing the prior authorization form.
How to Write
Step 1 – Begin by downloading the form in Adobe PDF and opening it up on your computer. The form has been made fillable online, but can also be printed out and filled in by hand if preferred.
Step 2 – The member information will be required first. Enter the patient’s first and last name, the plan they have with Catamaran, their member ID and their date of birth. Below this, the following drug information will be required:
- Drug name
- Quantity
- Directions
- ICD-9
- Directions
- Duration of therapy
- Diagnosis
Step 3 – The reasoning behind prescribing the drug should be provided in paragraph format. All pertinent medical information can be submitted in the fields below the “Medication/Failure Reason” paragraph.
Step 4 – Under “Physician Information,” submit the below data before printing the form off and providing your signature.
- Physician name
- Date
- NPI #
- Phone number
- Action needed (Urgent or For Review)
- Fax
- Pharmacy Fax
Fax the completed form to: 1 (888) 852-1832