Fidelis Prior Prescription (Rx) Authorization Form

The Fidelis Prior Prescription (Rx) Authorization Form allows a prescribing physician to request coverage for a prescription drug. This document is not required if the drug is already on the insurance provider’s formulary; however, should all other formulary medications prove insufficient in treating the patient’s illness, coverage for non-preferred/non-formulary drugs can be obtained. The prescriber will need to fill out the below form in full, providing all medical justification for requesting the specific drug. Once completed, it can be faxed to Fidelis Care. Generally a response can be expected within three (3) business days.
How to Write
Step 1 – Download in Adobe PDF to get started.
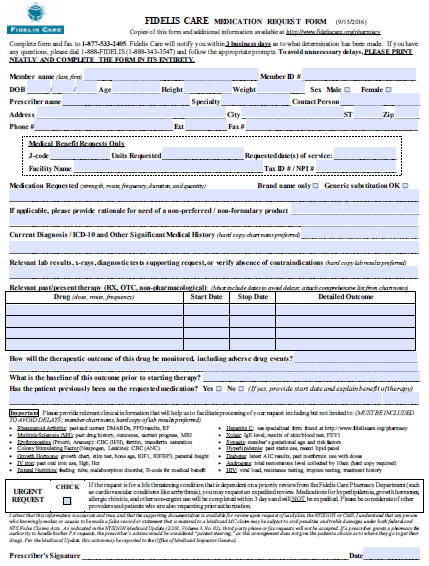
Step 2 – The first information required pertains to the member for whom coverage is being requested, as well as the individual prescribing the drug in question. Enter in the following data:
- Member name
- Member ID
- Date of birth
- Height
- Weight
- Sex
- Prescriber name
- Prescriber specialty
- Contact person
- Office address
- Office phone and fax numbers

Step 3 – If applicable, fill in the “Medical Benefit Requests Only” window with the following information:
- J-code
- Units requested
- Requested date(s) of service
- Facility name
- Tax ID #/ NPI #

Step 4 – Here is where the medical rationale for prescribing the non-preferred drug can be supplied. Enter the name of the medication requested and indicate whether or not the drug should be “Brand name only.” The rationale for the non-preferred drug can be provided in the second line. The current diagnosis and pertinent medical history can be supplied in the third line, while all other tests, x-rays and the like can be detailed in the fourth field.
Step 5 – Past/present therapies which have been prescribed should be indicated in this window. Include the drug dose, route and frequency in the first field, the start and stop dates in the second and third, as well as the detailed outcome in the forth.

Step 6 – Answer these three (3) final questions asking whether the outcome will be monitored, what the baseline of the outcome is prior to starting therapy, and whether the patient has been on requested medication already.

Step 7 – If this is an urgent request, check the provided box. When ready, print off the form, provide your signature and the date, and fax the completed document to 1 (877) 533-2405.