
Harvard Pilgrim Healthcare Prior Prescription (Rx) Authorization Form

The Harvard Pilgrim Healthcare Medication Request Form can be used for a number of purposes, one of which is prior authorization. Prior authorization allows the prescriber to request coverage for their patient prior to prescribing the preferred medication. Often this is required if the prescription drug being administered is atypical. The healthcare provider must complete the form in full, providing a list of previously applied treatments and their justification for requesting an alternative drug.
How to Write
Step 1 – Begin by downloading the Harvard Pilgrim HealthCare Medication Request Form in Adobe PDF. You can provide the requisite information by hand or on your computer.
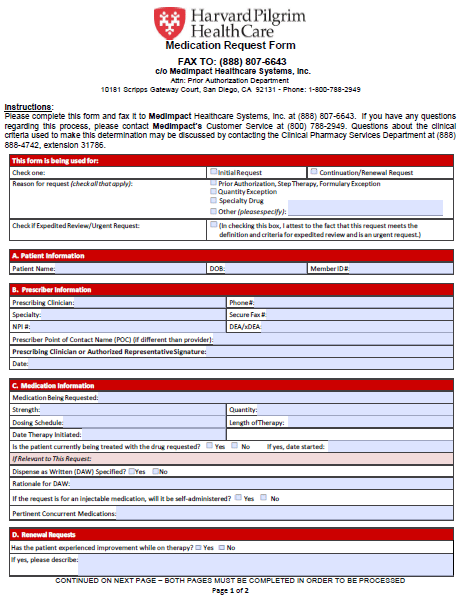
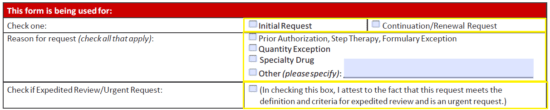
Step 2 – Identify the use of the form; whether it’s an initial request or a continuation/renewal request. Also signify the reason for the request and check the applicable box if the request is to be expedited.
Step 3 – In the first window, enter the patient’s name, date of birth, member ID #.
![]()
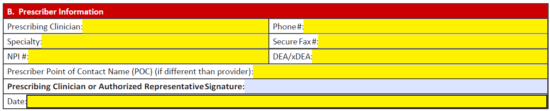
Step 4 – Section “B” requires the prescriber’s information. This will include all of the following info:
- Prescribing clinician
- Specialty
- NPI #
- Prescriber POC
- Phone number
- Fax number
- DEA/xDEA
- Date
- Prescribing clinician signature (after printing if applicable)
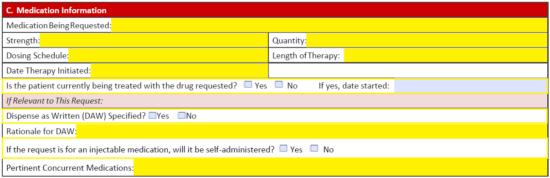
Step 5 – Now info on the requested medication can be supplied. Enter the medication name, strength, dosing schedule, quantity, length of therapy, and therapy start date to begin. Next, check “yes” or “no” to indicate whether the patient is currently being treated by the requested drug. If relevant to the request, supply the following:
- DAW specified (yes or no)
- Rationale for DAW (if applicable)
- Is medication injectable and to be self-administered (yes or no)
- Pertinent concurrent medications
Step 6 – If this form is being used for a renewal request, indicate whether or not the patient has experience improvement while on the prescribed medication. If yes, describe the improvements in the available field.

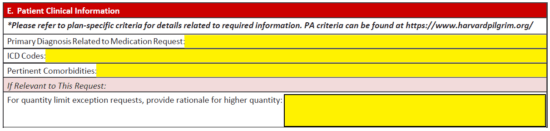
Step 7 – In Section “E,” enter in the below info.
- Primary diagnosis
- ICD codes
- Pertinent comorbidities
- For quality limit exception requests, provide rationale (if applicable)
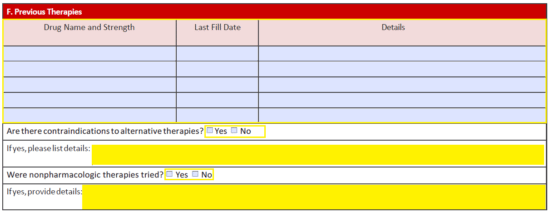
Step 8 – List all previous therapies, and then answer whether there are contraindications to alternative therapies. If yes, describe. If nonpharmacologic therapies were attempted, provide more information.
Step 9 – The relevant lab values must be supplied in this table along with the requisite documentation.

Step 10 – If the medication is a compound, check “Yes” and provide the ingredients. For any compound or off label use, include citation to peer reviewed literature where applicable.

Step 11 – Any additional information that may be useful in this request can be supplied in the final window. Print off the document once double checked for accuracy, provide the required signature, and fax the completed form to (888) 807-6643.
