
Medicare Prior Prescription (Rx) Authorization Form

The Medicare Prior Prescription Authorization Form or Medicare Part D Coverage Determination Request Form is used to request financing for a non-preferred medication by the insurance company in question. Some Medicare plans have their own specific document which they prefer to use; however, the below universal form can be sent to all Medicare providers. Once completed with all the patient’s and physician’s information, along with the rationale for prescribing a medication which is not on the formulary, the form can be faxed to the patient’s Medicare plan’s office for review.
How to Write
Step 1 – Download the document in Adobe PDF to start.
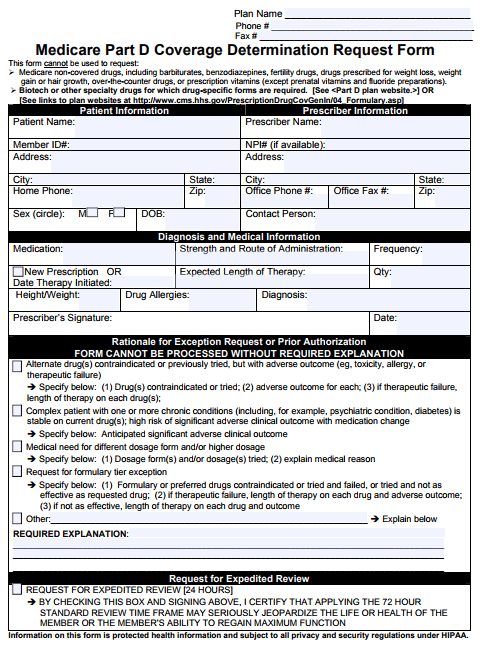
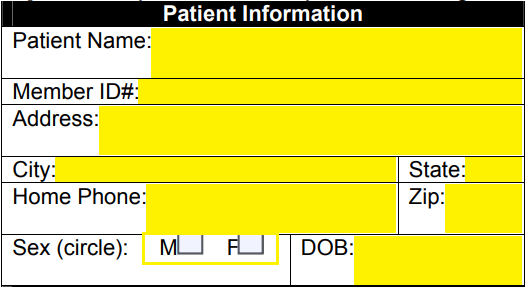
Step 2 – Under “Patient Information,” supply their name, member ID#, full address, phone number, sex, and date of birth.
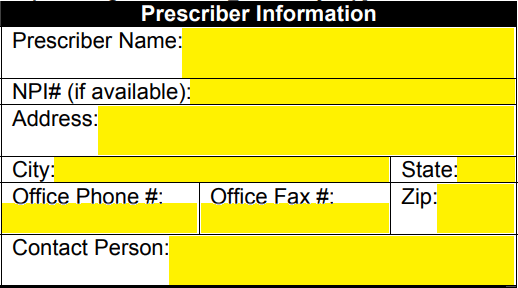
Step 3 – The prescriber’s full name, NPI number, address, office phone, office fax, and office contact person must be entered in the second window.
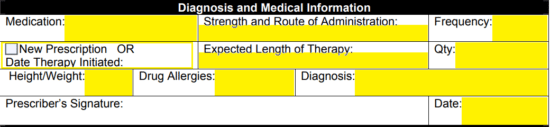
Step 4 – In the “Diagnosis and Medical Information” window, you will have to enter the following data:
- Medication
- Strength and route of administration
- Frequency
- New prescription or date of therapy initiated
- Length of therapy
- Quantity
- Height/weight of patient
- Patient drug allergies
- Diagnosis
Supply the day’s date where applicable but leave the prescriber’s signature field empty until the document has been printed.
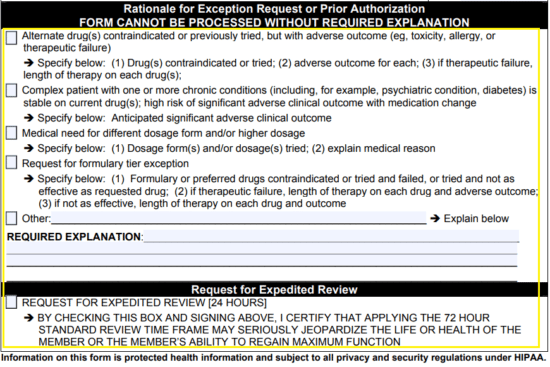
Step 5 – In this window, you will need to provide the rationale for prior authorization. Select the applicable box and if the rationale is not supplied under the first four (4) options, check the last box and provide the explanation below. If the document should be expedited due to the condition of the patient, check the appropriate box at the bottom of the form.
Step 6 – Print the document, provide your signature and fax the form to the patient’s healthcare plan to complete the process.