

The Medicare consent form is used when a Medicare beneficiary wishes to authorize the release of their medical information from the Center for Medicare and Medicaid Services to an entity or individual. This can be health information or information as it pertains to the settlement received. It should be noted that if the beneficiary wishes to release their information to more than one entity or individual, they will need to fill out a separate form for each.
How to Write
Step 1 – Download in Adobe PDF.
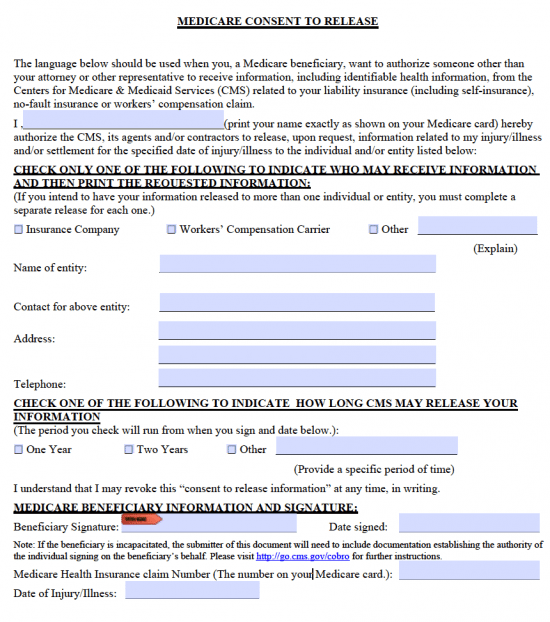
Step 2 – Read over the information in the first couple of paragraphs before submitting your full name as shown on your Medicare card.

Step 3 – Check one of the boxes here to indicate who can receive the information. If “Other,” explain. After this, provide the following:
- Name of entity
- Contact for above entity
- Address
- Phone number
Step 4 – Specify the amount of time CMS may release the information by checking “One Year,” “Two Years,” or “Other.” Enter in the specific period of time if “Other” was selected.
Step 5 – The date signed, health insurance claim number, and date of injury/illness can all be provided before printing and signing the document.
